

Bilateral Retrograde Pyelogram Cpt Code
For total functionality of this publication it is necessary to enable Javascript.
Click here to run across instructions how to enable JavaScript in your web browser.
Percutaneous Procedure CPT Code Update
Jonathan Rubenstein, MD
Chesapeake Urology Associates, Baltimore, Md
[Rev Urol. 2016;eighteen(i):38-43 doi: x.3909/riu0707]
© 2016 MedReviews®, LLC
Percutaneous Procedure CPT Lawmaking Update
Jonathan Rubenstein, MD
Chesapeake Urology Assembly, Baltimore, Doctor
[Rev Urol. 2016;eighteen(1):38-43 doi: 10.3909/riu0707]
© 2016 MedReviews®, LLC
Percutaneous Procedure CPT Lawmaking Update
Jonathan Rubenstein, MD
Chesapeake Urology Assembly, Baltimore, Physician
[Rev Urol. 2016;18(1):38-43 doi: 10.3909/riu0707]
© 2016 MedReviews®, LLC

A number of new and revised Common Procedural Engineering science (CPT®; American Medical Clan, Chicago, IL) codes pertaining to percutaneous renal access, renal drainage, and diagnostic and therapeutic procedures performed percutaneously were introduced on January ane, 2016. In addition, several commonly used CPT codes for percutaneous renal procedures were eliminated. The new and revised CPT codes for percutaneous procedures became necessary equally several of the older procedure codes were existence billed with the radiologic supervision and interpretation code in over 75% of cases and needed to exist bundled together. In add-on, there was a need for greater specificity due to unlike work requirements of unlike procedures that were previously captured inside one code. The new CPT codes for percutaneous renal access and drainage now include radiologic supervision and interpretation in the clarification. The new codes allow for more streamlined and simplified coding, and eliminate the prior need for multiple codes for a procedure that now can be captured with i code, or with fewer codes, due to their increased specificity. Urologists and interventional radiologists who perform percutaneous renal procedures must have a comprehensive understanding of these changes and the new, established, and eliminated codes to ensure accurate documentation and accurate coding.
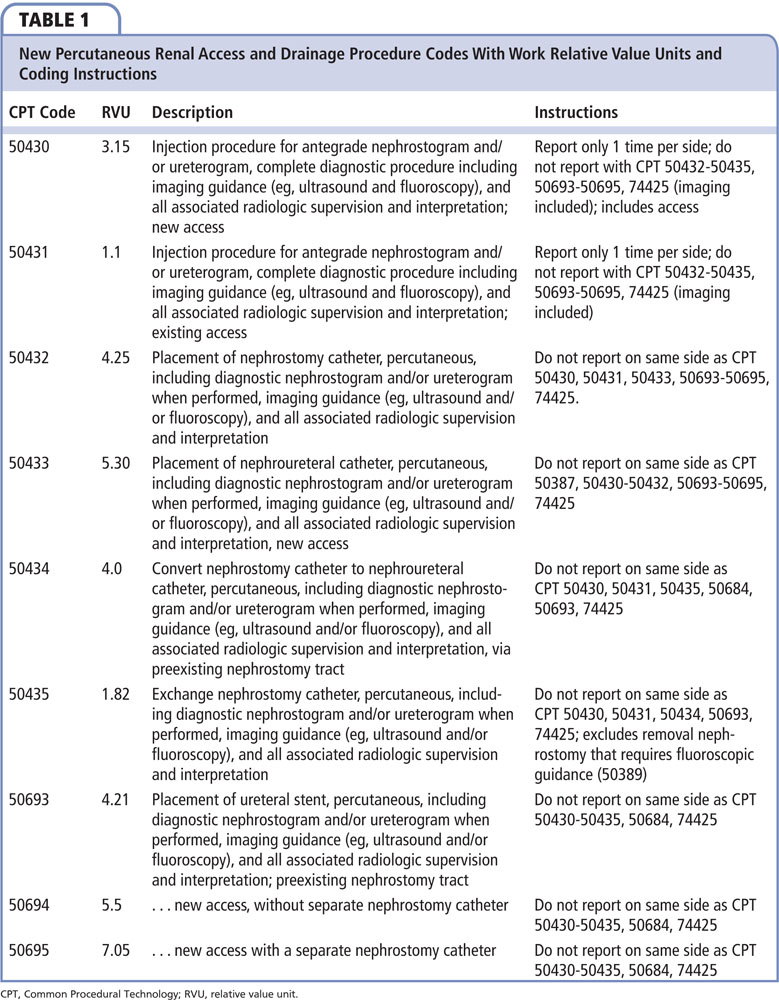
New Percutaneous Renal Access and Drainage Codes
New Codes
CPT 50430 Injection procedure for antegrade nephrostogram and/or ureterogram, complete diagnostic procedure including imaging guidance and all associated radiologic supervision and interpretation, new access; and CPT 50431 … through existing access (Table 1).
Eliminated Code
CPT 50394 Injection procedure for pyelography through nephrostomy or pyelostomy tube or indwelling catheter.
CPT 50394 (diagnostic injection) was beingness billed with CPT 74425 (radiologic supervision and interpretation) in more 75% of cases, which necessitated a new combination code. The two new codes include radiologic supervision and interpretation every bit part of the description, so an interpretation lawmaking should not exist separately coded. CPT 50430 should exist used when a new access is placed for injection, and CPT 50431 should be used if the injection is performed through an access that already exists. These codes should not be reported more than than once per accessed side, but tin exist billed with an appropriate modifier (if needed) if performed on reverse sides. As radiologic supervision and interpretation are included in the new CPT codes for placement of a nephrostomy tube, stent, or nephroureteral catheter, CPT 50430 and CPT 50431 should not exist coded in addition to the placement or commutation codes unless performed on reverse sides.
New Code
CPT 50432 Placement of nephrostomy catheter, percutaneous, including diagnostic nephrostogram and/or ureterogram when performed, imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation.
Eliminated Code
CPT 50392 Introduction of catheter into renal pelvis.
CPT 50392 (nephrostomy tube placement) was existence billed with CPT 74475 in more than 75% of cases, and so a new lawmaking was needed to bundle the procedures together. As image supervision and estimation are included in CPT 50432, an estimation code should not be used separately. Procedures performed on the opposite side or in a different location within the kidney can exist coded using the appropriate modifier. Injection for nephrostogram (CPT 50430 and CPT 50431) should not be coded if performed on the same side.
New Codes
CPT 50433 Placement of nephroureteral catheter, percutaneous, including diagnostic nephrostogram and/or ureterogram when performed, imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation, new admission.
CPT 50693 Placement of ureteral stent, percutaneous, including diagnostic nephrostogram and/or ureterogram when performed, imaging guidance (eg, ultrasound and/or fluoroscopy), and all associated radiologic supervision and estimation; preexisting nephrostomy tract.
CPT 50694 … via a new access without a separate nephrostomy catheter.
CPT 50695 … via new access with a separate nephrostomy catheter.
Eliminated Code
CPT 50393 Introduction of ureteral catheter or stent into ureter through renal pelvis for drainage and/or injection, percutaneous.
Replacement codes for CPT 50393 were deemed necessary due to the frequent coding with an interpretation code and due to need for increased specificity. Dividing this i code into 4 unique codes achieved more specificity and more accurate work values for payment. The placement of a nephroureteral catheter (CPT 50433) requires more work and effort and, therefore, has college work relative value units (RVUs) than nephrostomy tube placement (CPT 50432). The three codes for placing a ureteral stent through a percutaneous approach are divided on whether at that place is a preexisting nephrostomy tract (CPT 50693), whether new access is achieved merely no nephrostomy remains (CPT 50694), or whether new access is achieved and a nephrostomy is also placed (CPT 50695). One should not bill for an antegrade nephrostogram (CPT 50430 or CPT 50431) or the placement of a nephrostomy (CPT 50432) with whatever of these codes if performed on the same side.
New Codes
CPT 50434 Convert nephrostomy catheter to nephroureteral catheter, percutaneous, including diagnostic nephrostogram and/or ureterogram when performed, imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation, via preexisting nephrostomy tract.
CPT 50435 Substitution nephrostomy catheter, percutaneous, including diagnostic nephrostogram and/or ureterogram when performed, imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation.
Eliminated Code
CPT 50398 Change of nephrostomy or pyelostomy tube.
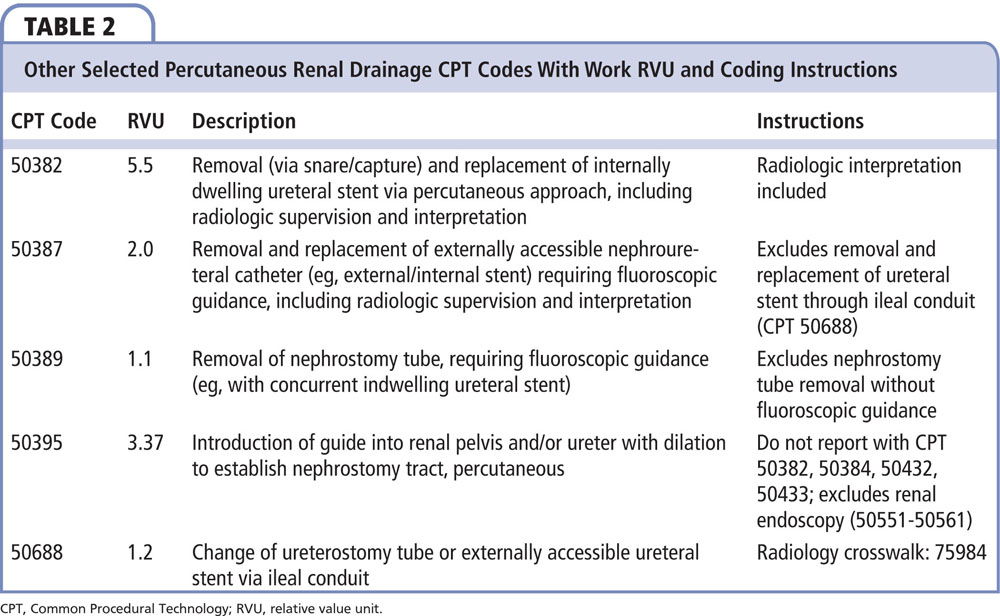
CPT 50398 was typically billed along with an interpretation code such equally CPT 74425, making a new arranged lawmaking necessary. The two new codes include converting a nephrostomy to nephroureteral catheter (CPT 50434), which requires more than work than exchanging a nephrostomy catheter (CPT 50435). Once again, one should not bill for an antegrade nephrostogram or placing or replacing a nephrostomy separately on the same side. Exchanging of a nephroureteral catheter for a new nephroureteral catheter is already captured using the already established CPT 50387 (Tabular array 2), although the terminology is updated, as previous language described a transnephric stent. This code includes radiologic supervision and interpretation. The removal and replacement of an externally accessible ureteral stent (such as an ileal conduit stent) is captured using CPT 50688.
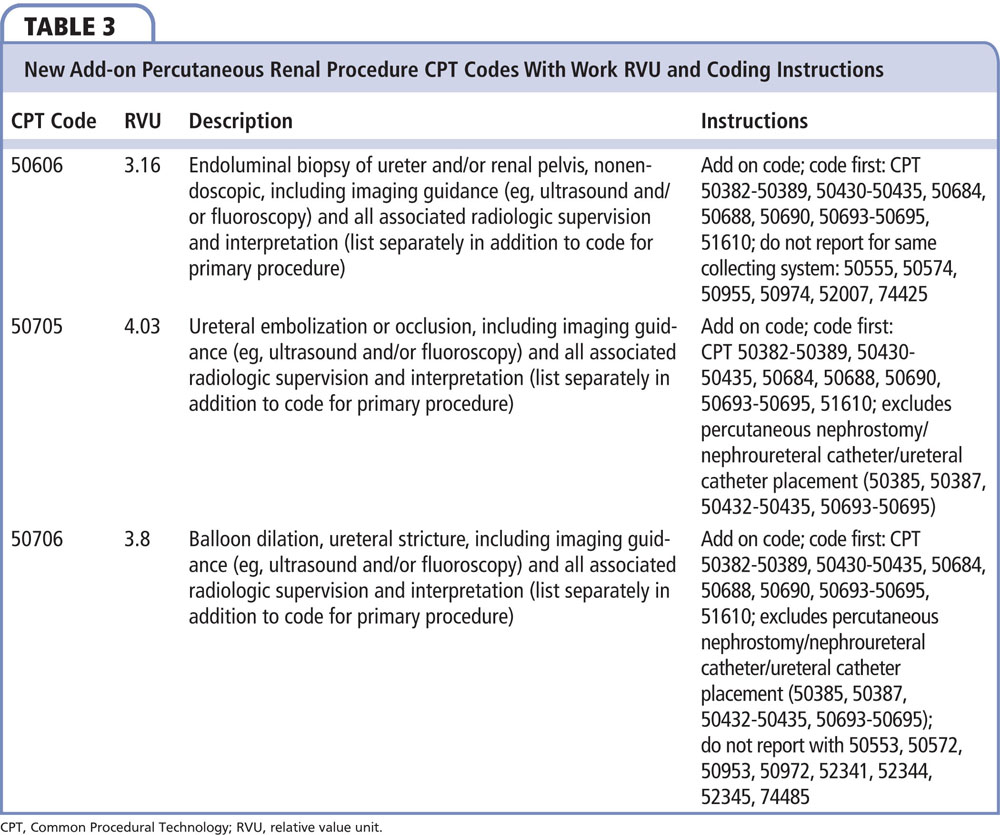
New Add-on Codes for Percutaneous Renal Procedure
In addition to new and updated percutaneous renal access and drainage codes, iii new percutaneous renal procedural codes were introduced (Table three).
CPT 50705 Ureteral embolization or occlusion, including imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation (list separately in addition to code for master procedure); CPT 50706 Balloon dilation, ureteral stricture, including imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation (list separately in addition to lawmaking for primary process); and CPT 50606 Endoluminal biopsy of ureter and/or renal pelvis, nonendoscopic, including imaging guidance (eg, ultrasound and/or fluoroscopy) and all associated radiologic supervision and interpretation (list separately in addition to code for principal procedure).
The 3 new percutaneous renal procedural codes listed are considered "improver" codes. For accurate coding, the access code for the procedure should exist billed first, and these addition codes billed afterwards. For percutaneous biopsy of a renal pelvis or ureter lesion, CPT 50606 should simply exist billed if straight visualization, such as using a nephroscope, is not performed. If the biopsy is performed nether directly vision, CPT 50555 is used if performed through a nephrostomy and CPT 50955 used if performed through an established percutaneous ureterostomy (Tabular array 4). Note that CPT 50574 and CPT 50974 are for open procedures (such as flank incision) to access the kidney and ureter for biopsy. Similarly, for ureteral dilation, CPT 50706 should only be used if endoscopy is not performed. If endoscopy is performed for ureter dilation then CPT 50553 should be reported if performed through a nephrostomy and CPT 50953 if through a ureterostomy (Table 4). CPT 50572 and CPT 50972 are used for open approaches to access the kidney and ureter (such as using a flank incision)
Common Scenarios for Billing for Urology
When billing for services provided, the outset and virtually important pace is authentic documentation. With the increased specificity of the currently available CPT codes, the provider who performs the procedure needs to specifically and accurately document in the note the presence or absenteeism of access prior to initiation of the case; any new admission that may be achieved during the example; the laterality; the procedure performed; and detail which tubes (if any) remain indwelling later the case.
Note that the code choices and rationale discussed herein are for advice but, are the most authentic codes bachelor for specific scenarios, only do not guarantee payment. Local insurer rules, including bundling and modifiers, should ever be followed. This is not an exhaustive list of all potential scenarios, just should serve as a starting indicate for proper coding.
Scenario 1: Percutaneous Nephrolithotomy With Percutaneous Access Already in Place
A commonly encountered scenario for urologists is the functioning of percutaneous nephrolithotomy for a stone > 2 cm (CPT 50081) in a patient with a nephrostomy tube already in identify. In addition to billing CPT 50081, the following CPT codes should be called: if the urologist uses the existing tract, performs the example, and replaces a nephrostomy at the stop of the case, it is most accurate to also bill CPT 50435 (removal and replacement of nephrostomy). If the surgeon converts the existing nephrostomy to a nephroureteral catheter at the end of the case, then the add-on code is CPT 50434 (convert nephrostomy to nephroureteral catheter via preexisting nephrostomy tract). If the patient has an antegrade double-J stent placed but is left without a nephrostomy, then CPT 50693 (placement of ureteral stent through preexisting nephrostomy tract) should be billed. If both a double-J stent and nephrostomy are placed, and so both CPT 50693 and CPT 50435 should be billed (CPT 50693 has higher RVUs and so is placed higher up CPT 50435).
If the urologist places a second (or third, or quaternary) admission in add-on to the existing access, so the following CPT codes should be added: CPT 50395 (Introduction of guide into renal pelvis and/or ureter with dilation to establish nephrostomy tract, percutaneous) if the access was used simply no nephrostomy remained in that access or CPT 50432 (Placement of nephrostomy catheter, percutaneous, including diagnostic nephrostogram and/or ureterogram when performed, imaging guidance [eg, ultrasound and/or fluoroscopy] and all associated radiologic supervision and interpretation) if a nephrostomy remains in place. In these situations, a modifier (such as Modifier 59 or Modifier XS) may be needed. It is reasonable to bill each code per each separate renal access, with the appropriate modifier.
Scenario 2: Percutaneous Nephrolithotomy in Which the Urologist Achieves His or Her Own Admission
Another mutual scenario occurs when a urologist places his or her own access for a percutaneous nephrolithotomy. If the urologist performs a cystoscopy with ureteral catheter placement with retrograde pyelogram with estimation, the CPT 52005 and CPT 74420 should be chosen. If the procedure is performed (CPT 50081) and the patient remains tubeless at the end of the instance, CPT 50395 (Introduction of guide into renal pelvis and/or ureter with dilation to constitute nephrostomy tract, percutaneous) should be chosen, in addition to the stone removal process code. If a nephrostomy is used for postoperative drainage, CPT 50432 (nephrostomy tube placement) should be used. If a nephroureteral stent is placed, then CPT 50433 is the correct choice. If a ureteral stent is placed, CPT 50694 should be used if the patient remains tubeless, and CPT 50695 should exist used if the patient has a stent and nephrostomy. Additional admission sites at unique locations within the same kidney should with billed with the appropriate modifier (such as Modifier 59 or Modifier XS) if necessary, based on insurance carrier rules.
Conclusions
The new CPT codes for percutaneous renal access, drainage, and diagnostic and therapeutic procedures have increased the specificity of coding and billing, simply have also streamlined the coding process. It is vitally important to understand the current CPT codes available to most accurately certificate the procedure performed, and to submit the virtually authentic CPT codes for reimbursement purposes.

Bilateral Retrograde Pyelogram Cpt Code,
Source: http://read.nxtbook.com/medreviews/urology/volume18no1/codingcorner_percutaneous.html
Posted by: leegrited.blogspot.com
0 Response to "Bilateral Retrograde Pyelogram Cpt Code"
Post a Comment